I read this when someone posted it on another corner of the internet. Presented at ATS 2014: A Successful Fiberoptic Transorbital Endotracheal Intubation In An Emergent Setting. The title sort of gives it away.
You can read the full text here.

I read this when someone posted it on another corner of the internet. Presented at ATS 2014: A Successful Fiberoptic Transorbital Endotracheal Intubation In An Emergent Setting. The title sort of gives it away.
You can read the full text here.
See below for the citations from today’s presentation.
If you’re interested in reading some of Dr. Gurpreet Dhaliwal’s publications on diagnostic reasoning, or some of his Clinical Problem Solving Articles (a series in the New England Journal of Medicine that he recommends the use of for cognitive / diagnostic “simulation”), you can look at all of his authored articles in PubMed here. He also gave a shout-out in his grand rounds (see below) to their new Interactive Medical Cases series, which is sort of like a gamified version of the CPS series. Very cool stuff– not all emergency medicine relevant, but a lot of them are.
You can also watch a wonderful 45 minute Grand Rounds presentation he gave, called From Good to Great, focused on strategies for striving towards expertise in diagnostic reasoning.
Pat Croskerry has written many more articles than the two cited below. If you’re interested in a module-based approach to improving diagnostic reasoning and combating bias, you can find that at the Society to Improve Diagnosis in Medicine website (https://www.improvediagnosis.org). Specifically, the modules in the Clinical Reasoning Toolkit provides a great overview of Croskerry’s research and ways to apply it in clinical practice.
Last but not least, here is a link to the recently-published book Avoiding Common Errors in the Emergency Department (2nd edition) that I mentioned at the end.
The title says it all. I referenced this article on shift tonight for probably the third time and had to post it here so that I could keep track of it — this is a review of radiographic imaging and approaches to workup/management of various foreign bodies in both pediatrics and adults. It’s an excellent overview — it’s not the answer to a very specific question I saw another group publish in the 90s by Ell and Sprig, that taught us that “only the bones from cod, haddock, cole fish, gurnard, lemon sole, monk fish, grey mullet and red snapper are well seen by soft tissue radiographic techniques” — but it is still very useful in keeping these things straight. It has helpful images, algorithmic approaches to various types of suspected ingestions, and lots of references for more detailed information and studies. I would love it if Annals of EM would publish more stuff like this, even if it comes from outside our direct field.
I recently cared for a patient who was an injection drug user who presented with fever, tachycardia, and redness/swelling of the forearm near an injection site. Her initial workup was remarkable for an elevated white blood cell count, hyponatremia to the high 120s, and hyperlactatemia. The patient was not eager to be hospitalized (as I have found is often the case with patients who inject drugs), and during our conversation about the risks:benefits of hospitalization and aggressive treatment with IV antibiotics and supportive care for what I felt was likely a very serious soft tissue infection with sepsis, I mentioned that the patient’s blood level of sodium was low and that I was concerned this was a serious and grave sign that their infection might be quite severe. When I went home after the shift, I wondered what that was founded on other than knowing that sodium was included in the LRINEC score and having had some experience in the past seeing patients with serious / necrotizing skin/soft tissue infections (SSTIs) who presented with hyponatremia.
I did a brief literature search and turned up a few articles, including one publication from one of our program’s recent graduates looking at our county hospital’s population of IVDU-associated STTIs.
Briefly, what I found in these articles was:
a.) Hyponatremia is a commonly-reported finding in patients with skin and soft tissue infections, and it seems to be found more commonly in patients with IVDU-associated infections. It was found in 41% of the patients from the Detroit group, 38% of the San Francisco group (compared to 27% of non-IVDU patients), and in the study looking specifically at necrotizing infections (from UCLA Harbor, with 31% of the 124 patients reporting IVDU) 56% of the patients had hyponatremia.
b.) When present, hyponatremia seems to be related to worse outcomes and is prognostically generally a bad sign. The group from SFGH did not report the association between low sodium and outcomes, but the group from Detroit and UCLA both showed significantly higher mortality in the patients with low serum sodiums at presentation.
Another question I asked myself was why do these patients get hyponatremia? I don’t think anyone knows for sure, but the authors from UCLA Harbor postulated the following in their paper:
Sepsis leads to increased muscle glucose uptake, increased lactate production and decreased utilization, an increase in the calculated ratio of muscle membrane permeabilities to Na+ and K+, and an increased intracellular Na+ concentration. These effects may be mediated by complement activation. In addition, sepsis has been linked to an increase in antidiuretic hormone level as well as adrenocortical insufficiency, both of which may lead to hyponatremia. Finally, severe NSTIs lead to marked third spacing of fluids, which may be replaced by free water, leading to hypovolemic hyponatremia.
I don’t know for sure how all this translates into clinical practice, but I do pay attention when I see low sodium in patients with infection, particularly if I’m concerned about how aggressive of a soft tissue infection this might be. But I also know that hyponatremia can be caused by heart failure, dietary deficiency, water intake, drugs, all sorts of things. It is a laboratory finding associated with so many different underlying actual problems, making it rarely useful in isolation. I’ve seen this often used as the reason for justifying admissions for patients with vague symptoms and many comorbidities but I think it is rarely the isolated cause of all of what the patient is experiencing. It’s also something that’s intimidating to be tasked with correcting in people, given the apparent stakes we learn about in medical school! It would be interesting to learn more about hyponatremia acts as a prognostic indicator in all those other conditions — I’m sure it isn’t good.
One of my senior residents, now graduated and a fancy informatics fellow and general badass at Stanford, Christian Rose and I used to discuss how we wondered if in extenuating circumstances one could use an intraosseous drill / needle to trephine a skull and drain a rapidly-expanding intraaxial hematoma in a crashing patients. Like most emergency medicine doctors, I find life-saving procedures interesting and cool and even though I would never want the lifestyle that accompanies neurosurgery, being able to do these interventions in a resource-limited setting is something I aspire to if it had to be done. (I’ve seen a burr hole and clot evacuation done once by an ED physician who had been trained in the military and done them abroad in forward operating theaters — he borrowed a drill from the ortho OR. It was successful, appeared fairly easy, and saved a life.)
This was all just theoretical until I read this post from the EMCore conference blog by Peter Kas. He relates a story recently published as a case report in Injury of using an EZ-IO drill and a 25 mm 15 ga intraosseous needle to drain a rapidly-expanding epidural hematoma in a pedestrian who was struck by an auto who presented and had a rapid decline in GCS and clinical signs of herniation. This procedure took about 8 minutes — shaving and sterilizing the scalp, and was done in the anesthesiology prep area while the neurosurgeons prepped for a craniotomy. They were able to aspirate ~ 30 mL of blood, with resulting improvement in the pupillary exam. A formal craniotomy was completed, and the patient had a good outcome.
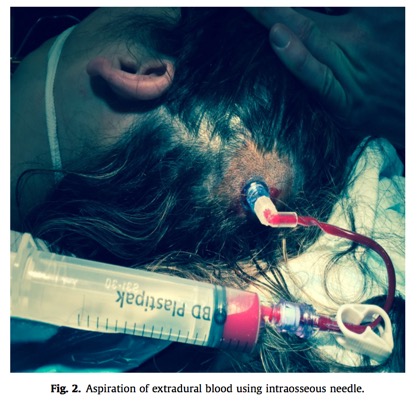
The authors note that this is unlikely to provide definitive management, given that most significant hematoma requiring craniotomy are of a more solid consistency that would be difficult to drain entirely via this route, but that it might be utilized by ED providers needing to transfer a patient over a long distance to definitive care. They specifically describe how they envision the procedure:
We propose the site of insertion should be the point of maximal clot depth and therefore localisation of the insertion point would be on a case by case basis. Most extradural haematomas requiring emergency craniotomy are of sufficient size that we postulate that failure to place the needle into the haematoma is unlikely but a potential complication.
Anyway, fun fact of the day, and perhaps someday (hopefully this will never come up) a last-ditch hail mary move that is a little easier and possibly safer/faster than borrowing a drill from your local orthopod and hoping you don’t go too deep.
I saw a patient recently that made me think about something an attending in medical school had told me — that in children perhaps even moreso than adults, a seatbelt sign on the neck was concerning for the presence of blunt vascular injury, e.g. dissection or pseudoaneurysm or some other kind of damage to the carotid or vertebral arteries, and that this meant you should strongly consider CT angiography in these patients.
The patient in question was well-appearing, otherwise neurologically totally intact, smiling and playful, and had strong pulses in all her extremities. But on the sides of her neck, initially concealed under the cervical immobilization collar, were two nasty-looking abrasions with underlying ecchymoses left by her five-point restraint seat. Did we need to order a CTA on this kid?
I turned to PubMed for some help with this question, and found this article by Desai and colleagues in which they reviewed ten years worth of data in which patients from a few months to 17 years underwent CT Aniography of the neck. There were 85 MVC patients, 42 had a documented cervical seatbelt signs, and none of these had BCVI (positive predictive value = 0). None of the 3 MVC patients who DID have BCVI had a documented cervical seatbelt sign. 22 MVC had “some form of soft-tissue injury to the neck that was not specifically listed as a seatbelt sign”. Of these 22 patients, the one who later died from “severe cerebral edema and hemorrhage with probable upper cervical cord transection, met multiple criteria (EAST criteria) for screening, including a GCS score of 3 and a C4–C5 fracture dislocation injury.”
While this is subject to the same problems as all retrospective database dregs, it is certainly reassuring to know that the majority of children with soft tissue injuries to the neck in an MVC do not end up having a cervical artery or carotid dissection, and that when those things exist, there are often other abnormal findings on exam (e.g. diminished GCS or focal neurologic deficits). This is consistent with other literature describing neurologic emergencies (which dissections in the neck often accompany) in the setting of trauma. My takeaway is that while a seatbelt sign (or any other mark) on the neck should make you consider blunt vascular injury, the idea that it mandates CT of the neck is not supported by this center’s experience and especially given the radiosensitivity of the developing thyroid clinicians should be thoughtful about their imaging in this context.
Imagine this scenario — a patient arrives in the ED, GCS 3, and is intubated for airway protection prior to the arrival of neurosurgery, who evaluates the patient and announces that the pupils are fixed and dilated, and laments that the pupillary exam is unreliable because the patient was given neuromuscular blocking agents, or paralytics to accomplish endotracheal intubation. Are they right? Does the use of depolarizing or non-depolarizing agents affect the pupillary light reflex?
I have heard multiple answers to this question, which often contradict each other, so I did some reading. I found one study from my home institution done by anesthesiologists and one done by emergency physicians that evaluated this prospectively. Andrew Gray and colleagues from UCSF did a prospective study of 20 patients receiving endotracheal intubation for elective surgery, and used pupillometry (a fun device invented here) to measure the PLR in patients randomized to saline, pancuronium or vecuronium. One thing I liked in their paper was the mention of the story of Scott Smith, a physician who self-administered curare to investigate its effects as an analgesic. He was found to be paralyzed but to have intact pupillary reflexes. They found that 100% of the patients in this series continued to exhibit intact pupillary light reflexes after administration of paralytics.
The second study by Caro et al. studied 94 emergency department patients undergoing rapid sequence intubation, with 67 receiving succinylcholine and 27 receiving rocuronium. In this series, which while small and single-center is probably more relevant to emergency medicine practice, two blinded physicians assessed patients for pupillary reflexes following administration of paralytics for RSI, approximately one minute after administration of medications. They too found preserved PLR in the vast majority of patients (91% of those getting succinylcholine and 100% of those getting Rocuronium). For a more exhaustive review and critical appraisal of this one, see the Annals of EM August 2011 Journal Club, in which this paper was covered.
So what to take away from all of this? If someone has a fixed/dilated pupil after the administration of paralytics, do not assume it is from the medication. It probably isn’t, at least according to these data. Induction medications and other agents (especially atropine) can obviously affect pupillary size, but any abnormal findings in the setting of the altered ED patient needing intubation should probably be attributed to badness, and not to the medications given for intubation.
Say that three times fast.
We had a challenging case in our emergency department recently involving a patient with a self-inflicted stab wound to the anterior chest, which resulted in a pericardial effusion, prompting concern for the development of tamponade. A challenging element of the case involved thinking about the patient’s stability, and the urgent/emergent need for operative intervention v percutaneous intervention v observation — how could we determine whether this patient was, in fact, in cardiac tamponade or on their way towards developing this condition?
A classic teaching is to assess for a pulsus paradoxus, or an exaggerated decrease in the arterial blood pressure with inspiration. Traditionally this is done using a stethoscope and manual blood pressure cuff (I will not try to spell the S-word). If the difference in BP between the first expiratory Korotkoff sound and the first Korotkoff sound that no longer disappears with inspiration (the pulsus) is greater than 10 mmHg, a pulsus paradoxus is present.
Has anyone ever checked for one of these, or has this technique become like with many other physical exam findings, something that people are aware of but don’t really know how to check for? I’m not sure — I personally have never checked for one, and reach for the ultrasound when trying to risk stratify patients with pericardial effusions. Is there an easier way, or one that doesn’t require PoC echo?
These authors evaluate the utility of pulse oximetry, or plethysmography in the assessment of tamponade. They suggest that the difference between the inspiratory decrease in the magnitude of the waveform and the expiratory increase has been shown to correlate with intraarterially measured pulsus paradoxus. Unfortunately it turns out that this finding is not pathognomic for cardiac tamponade — it is linked to a number of other conditions (e.g. elevated intrathoracic pressures from asthma), and may be absent in patients who actually have tamponade physiology.
The most relevant article to this particular case is probably the study from Stone et al., “Respiratory changes in the pulse-oximetry waveform associated with pericardial tamponade.” from 2006, when they measured phasic respiratory variability in the pulse-oximetry waveform of patients undergoing aspiration of pericardial effusions. They found that the degree of respiratory variability in the pulse-oximetry waveform was significantly increased in these patients compared to effusion-less patients, and increased with the hemodynamic consequences of the tamponade. When the effusions were aspirated and drained, the variability disappeared.
So, is this something to hang your hat on? Probably not useful entirely for ruling OUT pericardial tamponade, but in a patient with an effusion if you’re asked by the consultant you wake up in the middle of the night whether you’ve checked for a pulsus yet, this might be an easier way than busting out your manual BP cuff and Googling how to check one the traditional way.
I came across this piece from a 2008 issue of Neurology recently, and wanted to keep it here for posterity. The conclusions of the study were clearly communicated by the title: “The “sunglasses sign” predicts nonorganic visual loss in neuro-ophthalmologic practice.”
In this seminal article, Bengtzen and colleagues performed a prospective analysis of all patients wearing sunglasses in clinic, and patients receiving diagnoses of “non-organic vision loss”, which was a technical term new to me. They report on a number of co-variates of this diagnosis, including the wearing of sunglasses inside the exam room, alongside “highly positive review of systems, workers’ compensation claim, disability, and lawsuit”.
Specifically, the reported sensitivity of wearing sunglasses for non-organic vision loss (NOVL) was 0.46 (95% CI 0.33 to 0.59). The prevalence of NOVL in the entire study population was 4.3% but 79% in sunglasses-wearing patients. The specificity of sunglasses for the diagnosis of NOVL was 0.995 (95% CI 0.989 to 0.998).
I found this interesting if only because it supports existing stereotypes about the wearing of sunglasses indoors. The article does not comment on why this relationship exists, nor does it suggest that the performance characteristics of this finding allow you to use it to rule in or rule out true vision threats, but it does shed some light on the patterns that shape our practice and color our perceptions.
I’m rotating through a community emergency department this month, in which it seems like 40% of the patients I’m seeing have dizziness as some element of their constellation of chief complaints. This is one of the most difficult chief complaints to evaluate in emergency medicine — not only because people use the term “dizziness” to describe a multitude of subjective experiences, e.g. vertigo, syncope/presyncope, generalized weakness, anxiety, ataxia, or any sort of disturbance in mentation. Add in the barriers to effective communication that can accompany elder patients visiting an ED, such as language barriers + hearing/vision issues that accompany aging (imagine a translator on a video phone screaming at a patient who is extremely hard of hearing) and this becomes a tricky subject indeed.
To that end, I reviewed a paper published by a Korean group evaluating dizzy patients in their emergency department: Characteristics of central lesions in patients with dizziness determined by diffusion MRI in the emergency department, by Lee et al.
This was a retrospective review of 902 patients presenting to a single ED with a chief complaint of dizziness over six months. They looked closely at 645 patients (!) who recieved MRI imaging as part of their workup, which showed 23 patients (3.6%) having strokes, the majority in the posterior circulation. The authors then examined the characteristics that best predicted the presence of a central lesion.
Their findings? Predictably, advancing age brought with it a higher likelihood of central etiologies: the rate of central lesions on DWI was 3.9% and 3.5% in patients in their 50s and 60s respectively; 7.4% in 70s and 16.7% in their 80s! Hypertension was more common in patients with strokes (69% versus 36%). Atrial fibrillation was more common. 77% of patients with a central cause reported a more vague non-whirling dizziness compared to 40% in patients without central lesions. Other associated neurologic symptoms were present in about 46% of patients with a central cause, compared to only 3% in those who were MR-negative.
So while this study had all the drawbacks of most retrospective, single-center publications, and may not generalize exactly to the populations I work with, I felt it was useful in terms of giving me at least *some* numbers to use to estimate what proportion of these patients are hiding badness. I will have a much lower threshold to MRI patients who are in their 70s-80s, those with AF who aren’t anticoagulated (though the sensation of palpitations or the diminished cardiac output can contribute to the sensation of dizziness as well), or those who report a “vague non-whirling” sense of dizziness. That last point stands in contrast to what I’ve read in other studies that suggested that the character of dizziness was *not* useful, so that was interesting. When this study was reviewed on EMRAP another thing that Sanjay and Mike mentioned was that older patients often have difficulties cooperating with the exam, accurately reporting/describing their symptoms, and that our threshold for obtaining further diagnostic imaging in these patients should be lower.
More on dizziness to come soon, I’m sure.