
One of my senior residents, now graduated and a fancy informatics fellow and general badass at Stanford, Christian Rose and I used to discuss how we wondered if in extenuating circumstances one could use an intraosseous drill / needle to trephine a skull and drain a rapidly-expanding intraaxial hematoma in a crashing patients. Like most emergency medicine doctors, I find life-saving procedures interesting and cool and even though I would never want the lifestyle that accompanies neurosurgery, being able to do these interventions in a resource-limited setting is something I aspire to if it had to be done. (I’ve seen a burr hole and clot evacuation done once by an ED physician who had been trained in the military and done them abroad in forward operating theaters — he borrowed a drill from the ortho OR. It was successful, appeared fairly easy, and saved a life.)
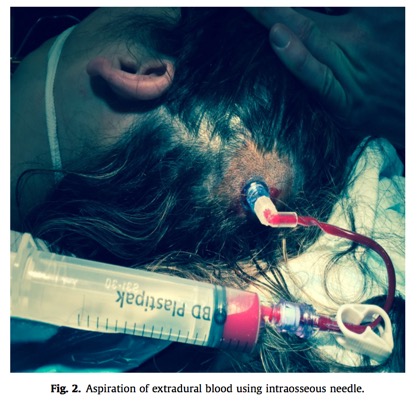
This was all just theoretical until I read this post from the EMCore conference blog by Peter Kas. He relates a story recently published as a case report in Injury of using an EZ-IO drill and a 25 mm 15 ga intraosseous needle to drain a rapidly-expanding epidural hematoma in a pedestrian who was struck by an auto who presented and had a rapid decline in GCS and clinical signs of herniation. This procedure took about 8 minutes — shaving and sterilizing the scalp, and was done in the anesthesiology prep area while the neurosurgeons prepped for a craniotomy. They were able to aspirate ~ 30 mL of blood, with resulting improvement in the pupillary exam. A formal craniotomy was completed, and the patient had a good outcome.
The authors note that this is unlikely to provide definitive management, given that most significant hematoma requiring craniotomy are of a more solid consistency that would be difficult to drain entirely via this route, but that it might be utilized by ED providers needing to transfer a patient over a long distance to definitive care. They specifically describe how they envision the procedure:
We propose the site of insertion should be the point of maximal clot depth and therefore localisation of the insertion point would be on a case by case basis. Most extradural haematomas requiring emergency craniotomy are of sufficient size that we postulate that failure to place the needle into the haematoma is unlikely but a potential complication.
Anyway, fun fact of the day, and perhaps someday (hopefully this will never come up) a last-ditch hail mary move that is a little easier and possibly safer/faster than borrowing a drill from your local orthopod and hoping you don’t go too deep.