
While I want to focus this blog on things relevant to practice in the Emergency Department, I have an academic interest (and maybe a career interest long-term) in critical care. I also feel that cardiac arrest is a particular area in critical care should be something that EPs are expert in — it’s also an area in which there is considerable nihilism which may lead in sub-optimal patient care, or early withdrawal of efforts before such withdrawal is justifiable.
What do I mean by nihilism? I mean that we in the ED rarely see good outcomes in out-of-hospital cardiac arrest (OOHCA) patients (and when we do, they’re often comatose and whisked away to the ICU, which means that even if they *do* have a good clinical outcome we do not see it happen and rarely even hear about it), and this leads to a sentiment that any cardiac arrest patient is bound for either death or a meaningless life due to neurologic injury.
Everyone in in the department, from patient care assistants and techs and medical students to the attendings, puts a lot of energy and effort into running codes and trying to resuscitate these patients. People care a lot and do some of their best work in these stressful contexts. But at the same time, I sometimes wonder whether we would focus more on improving our process and quality of care– and perhaps thereby do even better– if we had a better sense that our interventions translated into patients who could again be alive and well because of them. This sense is difficult to come by if many of the patients that you successfully attain ROSC on have features that many people associate with a very low likelihood of meaningful recovery.
This pair of recent review articles focused on prognostication in post-cardiac arrest patients — findings on clinical exam, imaging, and other methods to try to suss out who will go onto do well and who is unlikely to ever regain meaningful neurologic function. As ICU bed availability dwindles and the incidence of cardiac arrest and survival thereof continues to increase, this will be of increasing relevance to ED docs, intensivists, and those working with these patients.
So what is a “good outcome”? As the article says, “Experts in coma prognositication defined outcome by cerebral performance categories (CPCs; CPC 1 back to baseline, CPC 2 moderate impairment, CPC 3 severe impairment, CPC 4 vegetative or comatose, CPC 5: dead).” They bifurcate these into either a good (CPC 1 or 2) or poor (CPC 3-5) outcome. Obviously the difference between “moderate” and “severe” impairment is somewhat subjective, but there are additional tools used to help with this distinction.
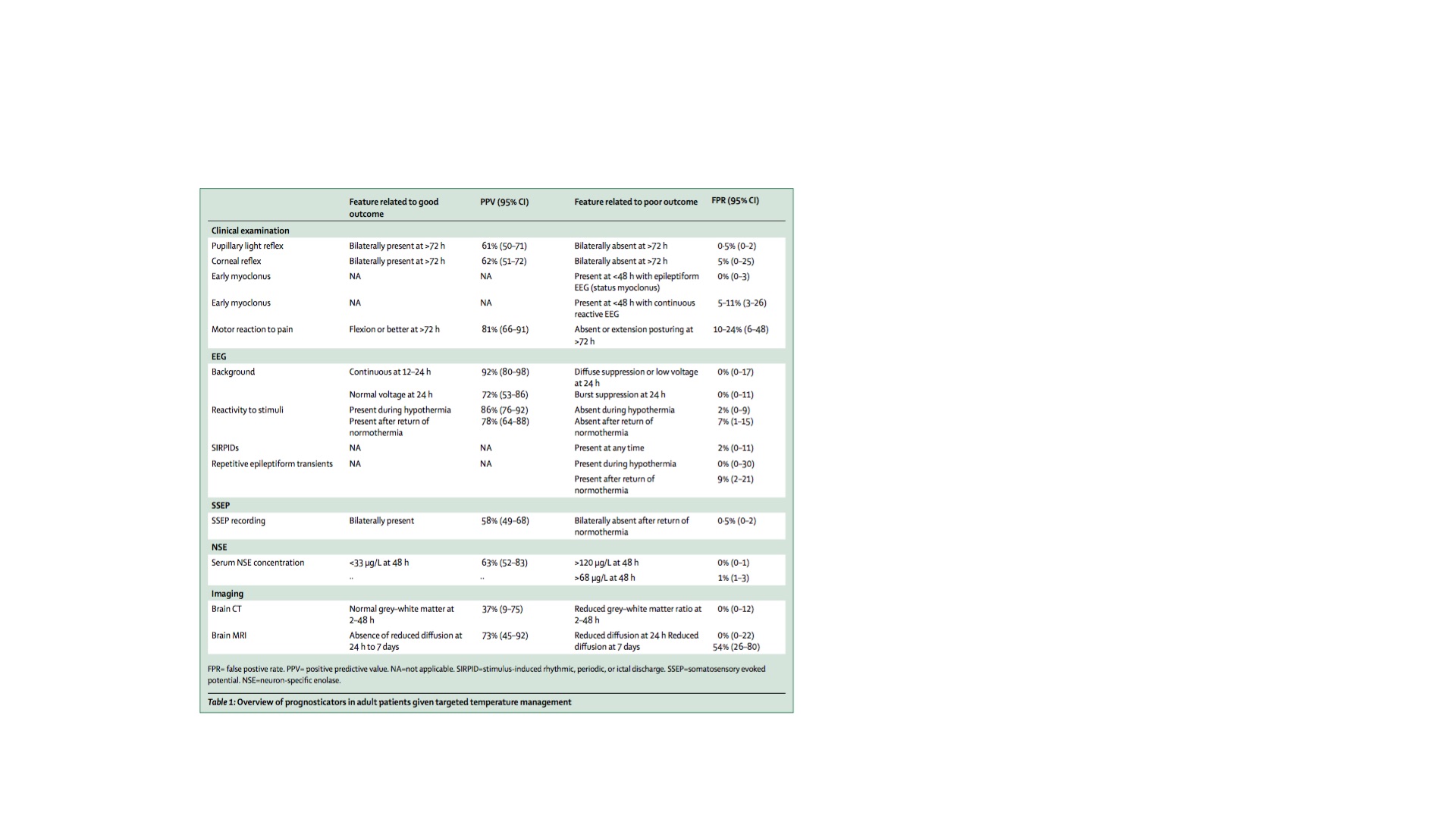
The old standard was clinical assessment of brainstem reflexes, the response to pain, and the absence or presence of myoclonus during the first 72 hours post-arrest. In the TTM era, this becomes trickier because temperature management and the required sedation can alter these features, though the bedside exam still has significant prognostic significance. Absence of pupillary reflexes at 72 hours is the best bedside predictor of a bad outcome, with a false positive rate (FPR) of only 0.5% — presence of pupillary reflexes however, does not confer a good outcome, given that it only has a PPV of 61% (95% CI 50-71).
What about earlier? In the first 24 hours post-arrest, particularly in hypothermic patients, ~ 8% of patients without pupillary reflexes will go on to have a good recovery — so don’t count them out. In terms of corneal reflexes, the reliability is less than that of pupillary reflexes but their absence still correlates with a poor prognosis, with an FPR of 5%.
Motor response is the most affected by sedatives, opiates, and neuromuscular blockade — all common in patients undergoing TTM, and absent or extensor responses to painful stimuli at 72 hours had a FPR of 24%. To reliably utilize this for prognostication, you need exclusion of residual effects of sedation, which can be extended beyond when the drips are simply turned off secondary to the effects of TTM and also the effects of reduced clearance due to shock liver, renal dysfunction, or both.
In terms of myoclonus, which is classically associated with poor outcomes, ~ 9% of patients with myoclonus may survive, according to the data presented here. As the article states, myoclonus is somewhat of a nebulously defined entity — “Not all so-called twitches have the same prognostic implication, rather their usefulness in predicting prognosis depends on semiology, duration, and associated EEG findings.”
I’ll skip EEG and ERPs because this is already too long, but suffice to say they’re useful after hypothermia and for ruling out sub-clinical status epilepticus, which is something we really want to avoid happening in our post-arrest patients, but is very common. More to come on this, which I feel is of particular relevance to us in the ED. Same goes for biomarkers such as neuron specific enolase and Serum S-100B, which can both be measured and trended as the “troponins of the brain”, so to speak.
In terms of imaging — CT scan of the head is recommended in patients in whom there is not another obvious cause of cardiac arrest, to evaluate for a bleed or ischemic stroke. Evaluation of gray:white ratios can predict poor outcomes, but is less reliable than clinical exam and EEG, and this is true for MRI as well, though again MRI does not add very much prognostic capability beyond what can be achieved with bedside tests and the logistics and cost associated with MRI scans of every comatose survivor of cardiac arrest make this somewhat limited in utility.

So what’s the takeaway from all this? Basically, reliable prognostication after cardiac arrest is hard, but at the same time, it isn’t– don’t do it right away, and if you do, it shouldn’t necessarily be based on your bedside neurologic exam. There are tools that can give us useful information, but rarely certainty, to guide conversations with family. And the reality is that none of them are accurate enough inside the first 48-72 hours, especially in patients who are being cooled. There is a very powerful desire to be able to give families hope, or to caution against hope in a way that changes outcomes before they’ve happened — in my very early-in-development opinion, all you can really tell them is something I heard one of my mentors say to families whose children were in the Pediatric ICU: “Prepare for the worst, and hope for the best.”
I also take away from this that nihilism is an un-useful form of prognsotication in these patients — I have seen patients myself who had unreactive pupils or myoclonic jerks, who went onto walk out of the hospital, fairly neurologically intact. This is even more true if the arrest was witnessed, was a shockable rhythm such as VT or VF, and if the patient received high-quality chest compressions and early defibrillation, preventing lengthy low/no-flow states to the brain.
The message not to take away from this post that I believe in any sense that there is no ability to meaningfully make predictions about the likely outcome of cardiac arrest patients, whether or not you’ve gotten ROSC — there are many other variables not considered in the above article that predict do reliably predict outcomes such as comorbidities, age of the patient, how long they were down for, the initial rhythm, and an often-overlooked variable in the literature (because it’s tough to quantify): consideration of their quality of life before they suffered a cardiac arrest. I also think that the pragmatic realities of cardiac arrest care — an emotionally charged event where patients are often teetering along a line between life and death, and where decisions have real and immediate impacts on that outcome– may require a sense of somewhat-morbid realism when the outcomes are often so dismal. I just hope that when people are making decisions about termination of efforts (or withdrawal of care post-ROSC) they’re considering all of these things and more, beyond just what their clinical gestalt is.
More to come, I’m sure — I’m especially interested in what happens moving forward in terms of biomarkers, cerebral oximetry, and near-infrared brain imaging to try to determine cerebral oxygenation and metabolism without having to move patients out of the ICU.


{kind=link}